1 Introduction
There are many known strategies for housing unsheltered people with serious mental illness. For decades, literature has demonstrated the efficacy of the “housing first” approach, which entails providing supportive housing before requiring treatment for substance use or mental health (1–8). Yet even cities that have made substantial investments in housing continue to find that addressing chronic unsheltered homelessness among people with serious mental illness is challenging. One reason that homelessness in this group persists despite policy efforts may be the dynamics of homelessness. In all populations, including those with serious mental illness, people move in and out of housing. In a simple model, adding a certain number of housing units, e.g., 2,000, would reduce the chronic unsheltered census by the same number (2,000). However, the presence of these dynamics complicates outcomes and makes it more difficult to estimate the number of units needed to reduce the size of the unsheltered population by a given number. A second challenge is that even when offered housing, some people, particularly those with serious mental illness, are not able to make a sustained transition to stable housing (9). Policies to enhance retention in housing may help this group remain in housing.
One reason that homelessness in this group persists despite policy efforts may be the dynamics of homelessness.
To assess how the dynamics of homelessness and the challenges of keeping people housed affect where people with serious mental illness are living, we developed a Markov model of housing and homelessness. A Markov simulation model is a stochastic, dynamic simulation that captures transitions across states across different time periods (10). This approach allows us to take into consideration that chronically unsheltered homelessness among people with serious mental illness is not a static condition (11). Over time, some housed people with serious mental illness become homeless; others exit homelessness for shelter (12). We calibrated our model to the population of adults with serious mental illness in New York City and simulated the effects on housing circumstances under alternative options for those in this group who live persistently on the streets for more than 2 years (a state we refer to as chronic unsheltered homelessness).
To assess how the dynamics of homelessness and the challenges of keeping people housed affect where people with serious mental illness are living, we developed a Markov model of housing and homelessness.
2 Prior Research
Although there are many point-in-time (PIT) counts of the homeless population and there is a robust literature on Housing First and similar interventions (1, 12), most of this literature does not address the challenges of transitions into and out of homelessness. Two prior longitudinal studies using Markov models provide information on usual sleeping place over time and the rates at which people enter and exit different types of places—transition probabilities (13, 14). Alexander-Eitzman’s analysis of the SUNCODA study in St. Louis, Missouri, reports on patterns of housing transitions for an urban population experiencing homelessness (13). Lemoine and colleagues uses the French Un Chez Soi d’Abord randomized clinical trial data to assess the cost effectiveness of Housing First combined with assertive community treatment (ACT) compared with usual care (in which housing was typically conditioned on mental health/substance use treatment) for a chronically unhoused population with serious mental illness (14).
Few studies have addressed the capacity of housing services needed to make substantial long-term changes in homelessness.
Few studies have addressed the capacity of housing services needed to make substantial long-term changes in homelessness. One prior study used randomized controlled trial data from the U.S. (HUD-VASH) experiment and the Canadian At Home/Chez Soi study and found, as we do, that although program capacity expansions reduced PIT counts in homelessness, the reduction over time was not one-to-one (15).
3 Data and Methods
We constructed a Markov simulation model in Microsoft Excel with four states: general housing (housed or in institutions or dead), unsheltered homelessness, sheltered homelessness, and newly provided supportive housing (13, 14, 16). Our analysis population consisted of all individuals with serious mental illness in New York City. We derived our initial baseline transition probability (rates at which people move from one state to another) estimates from the studies by Lemoine and colleagues (14) and Alexander-Eitzman and colleagues (13), using a 1-year cycle length and a 60-year time horizon (13, 14). However, as these studies do not fully correspond to the situations we are considering, we adjusted these probabilities and calibrated the model so that after 60 iterations, it produces baseline estimates consistent with outside evidence about the PIT housing of people in New York. In a sensitivity analysis, we used unadjusted transition probabilities from research in other settings. Our study was conducted from May through September 2022. Institutional review board approval was not obtained because the study did not involve human subjects research.
Population
We assumed, based on a review of the literature, that the New York City population with serious mental illness at risk of losing housing is 45,000 people. This figure is consistent with an underlying prevalence of serious and persistent mental illness that poses a risk of losing housing of 0.85% in nonelderly adults and an adult population of 5.3 million in New York City in 2022 (17–19). Our model conclusions are not substantially changed if we assume a larger (or smaller) initial count of people with serious mental illness at risk of losing housing, because we ultimately calibrate this figure nd rate to our estimates of the number of people with serious mental illness who are unhoused.
We assumed, based on a review of the literature,that the New York City population with serious mental illness at risk of losing housing is 45,000 people.
General housing (includes institutions and mortality). We assumed that most individuals (38,000) with serious mental illness at risk of losing housing are initially housed (for example, living with family or in institutions). This housed population included people living in existing NYC supportive housing (we did not separate out this population). It also included a relatively smaller number of people housed in other institutional settings, including hospitals, jails, or institutions (20–24). Finally, we treated mortality as a transition into the general housing state (although, of course, mortality is an absorbing state); implicitly, we assumed that the increase in the population of people with serious mental illness who become newly at risk for homelessness matches the decline in the population that occurs as people who are homeless die.
Chronic unsheltered homelessness. Based on consultation with a knowledgeable NYC official, we assumed that initially about 2,500 single chronically homeless adults with serious mental illness live on the streets of New York City. We refer to this group as “chronically unsheltered homeless.” The model operationalizes the chronicity of unsheltered homelessness by assigning low transition probabilities of exit to all other states.
Sheltered homelessness. We assumed the sheltered population with serious mental illness lives primarily in shelters and intermittently on the street; for brevity, we refer to this state as “sheltered homelessness.” We assumed, based on NYC PIT counts, that there are 4,500 sheltered people with serious mental illness in this category at baseline. In total, this yields a homeless population with serious mental illness of 7,000 people (24–30).
Interventions
After calibrating the base case to match observed data, we modeled three types of interventions. The initial intervention adds 2,000 units of supportive housing (31). To model this intervention, we adjusted our baseline transition probabilities such that 2,000 people live in new supportive housing in the new steady state. We allowed transitions into supportive housing only from the chronically unsheltered homeless state. This assumption is much more restrictive than the typical experience documented in prior studies, where some people entered supportive housing directly from other states (such as shelter). In our base case analysis, we assumed that the risk of transitioning into the general housing state is higher for those in chronic unsheltered homelessness than for those in (relatively more stable) supportive housing.
We allowed transitions into supportive housing only from the chronically unsheltered homeless state.
Next (intervention 2), we supplemented supportive housing units with complementary services aimed at improving housing retention (32, 33). We did this by increasing the transition probability around remaining in supportive housing.
Finally, we supplemented housing and retention interventions with a hypothetical preventive intervention that also addresses those who are housed at baseline. We present this case to illustrate the interaction between having a fixed number of supportive housing units and reducing the flow into chronically unsheltered homelessness. We modeled this preventive intervention (intervention 3) by increasing the probability of remaining in general housing.
Sensitivity Analyses
We conducted four sensitivity analyses in total. In three one-way sensitivity analyses, we simulated how much our conclusions would change if we modified our transition assumptions in intervention 1 (supportive housing only). A final sensitivity analysis simulated changes to the base case.
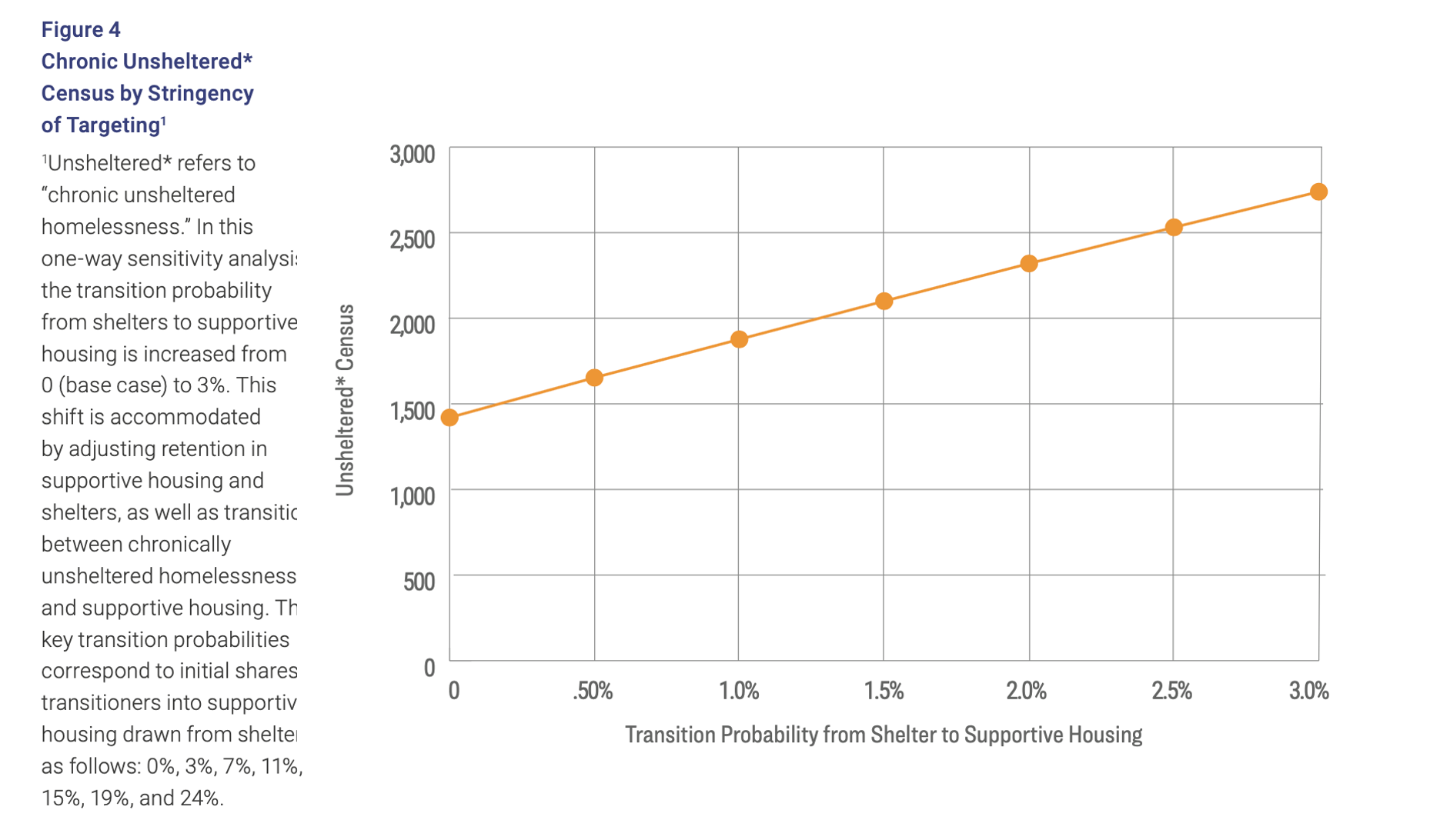
In our first sensitivity analysis, we modeled the effects of modifying our very restrictive assumption that new units are targeted only to people who have been in chronically unsheltered homelessness. Instead, we allowed up to 3% of those in sheltered homelessness to transition to supportive housing units.
Next, we modeled the effect of modifying our assumption that, relative to those who are chronically unsheltered, those who live in supportive housing have a lower rate of transition to the general housing state. We did this by increasing the transition rate for those in supportive housing (from 5%) to be the same as the rate for the chronically unsheltered (4).
Third, we modeled the effect of decreasing the fraction who are retained in supportive housing from our base case estimate of 75% down to 50%.
These studies reported much higher rates of exit from homelessness and supportive housing into general housing and institutions than we assume.
Finally, we separately simulated a model with assumptions across transitions that are closer to those in prior studies of supportive housing (e.g., Lemoine and colleagues [14] and Alexander-Eitzman and colleagues [13]). These studies reported much higher rates of exit from homelessness and supportive housing into general housing and institutions than we assume. These transition rates are so high that we needed to adjust downward (from 45,000 to 22,500) our assumptions about the underlying size of the population at risk for homelessness to generate a steady state of 4,500 people in shelters and 2,500 people experiencing chronic unsheltered homelessness.
4 Results
Figure 1 provides our base case transition probabilities. These transition estimates are calibrated to generate steady state totals of shelter and chronically unsheltered homeless people corresponding to the assumptions described above.
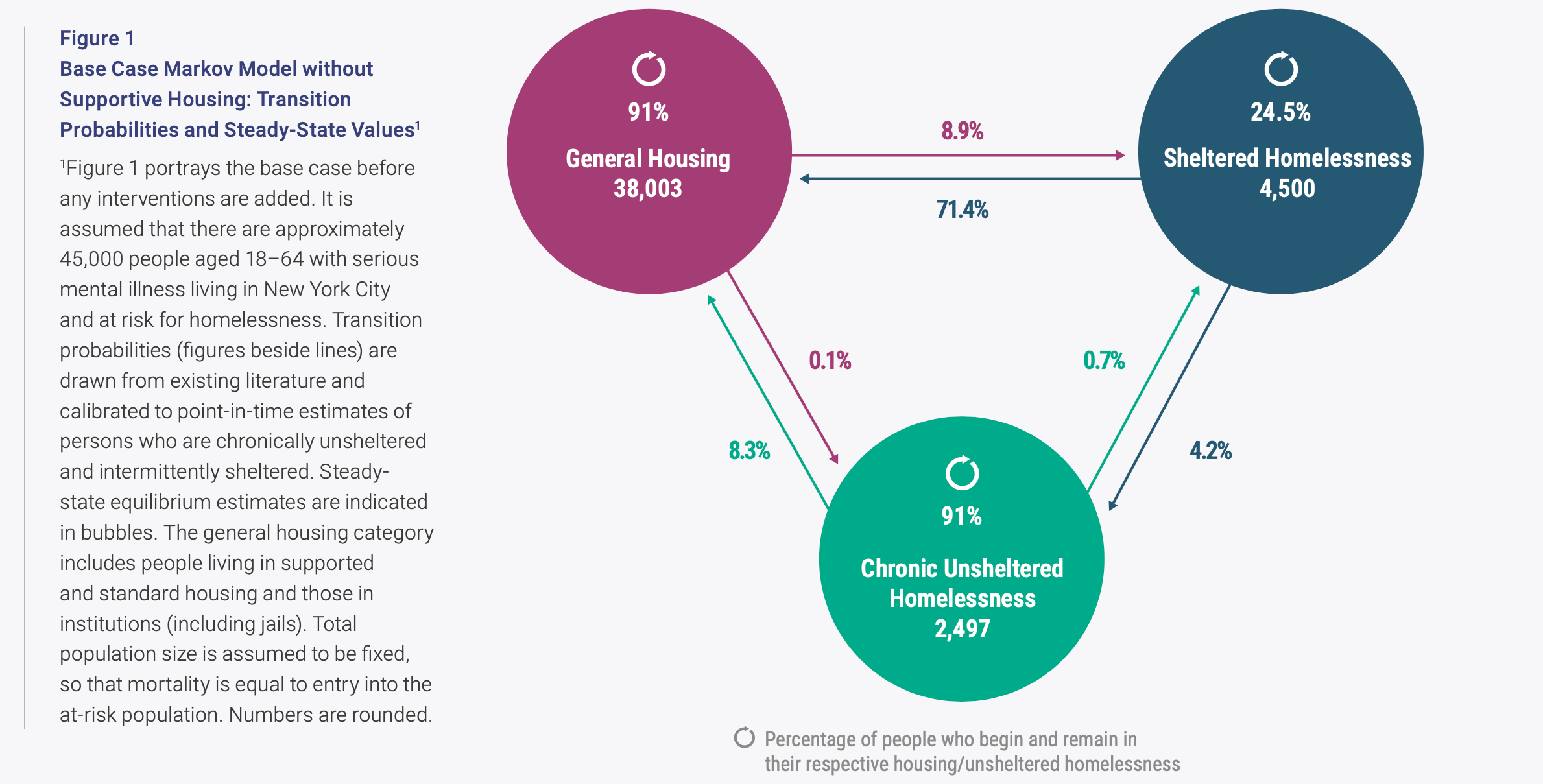
The number in the top left indicates that 91% of people who begin in general housing remain in general housing the following cycle. The figure on the arrow leading from general housing to sheltered homelessness indicates that 8.9% of those who begin in housing transition to sheltered homelessness in the following year. Finally, 0.1% of people who begin in general housing transition to chronic unsheltered homelessness.
Among those who begin in shelters, 71.4% transition to housing. About 24.5% remain in shelters, and 4.15% move to the streets. Among those who begin in chronically unsheltered homelessness, 8.3% move to housing, die, or become institutionalized; 0.7% move to shelters; and 91% remain in chronic unsheltered homelessness. The figures in the bubbles show the steady-state outcomes after 60 model iterations: 2,497 people are chronically unsheltered and 4,500 are in sheltered homelessness.
Interventions
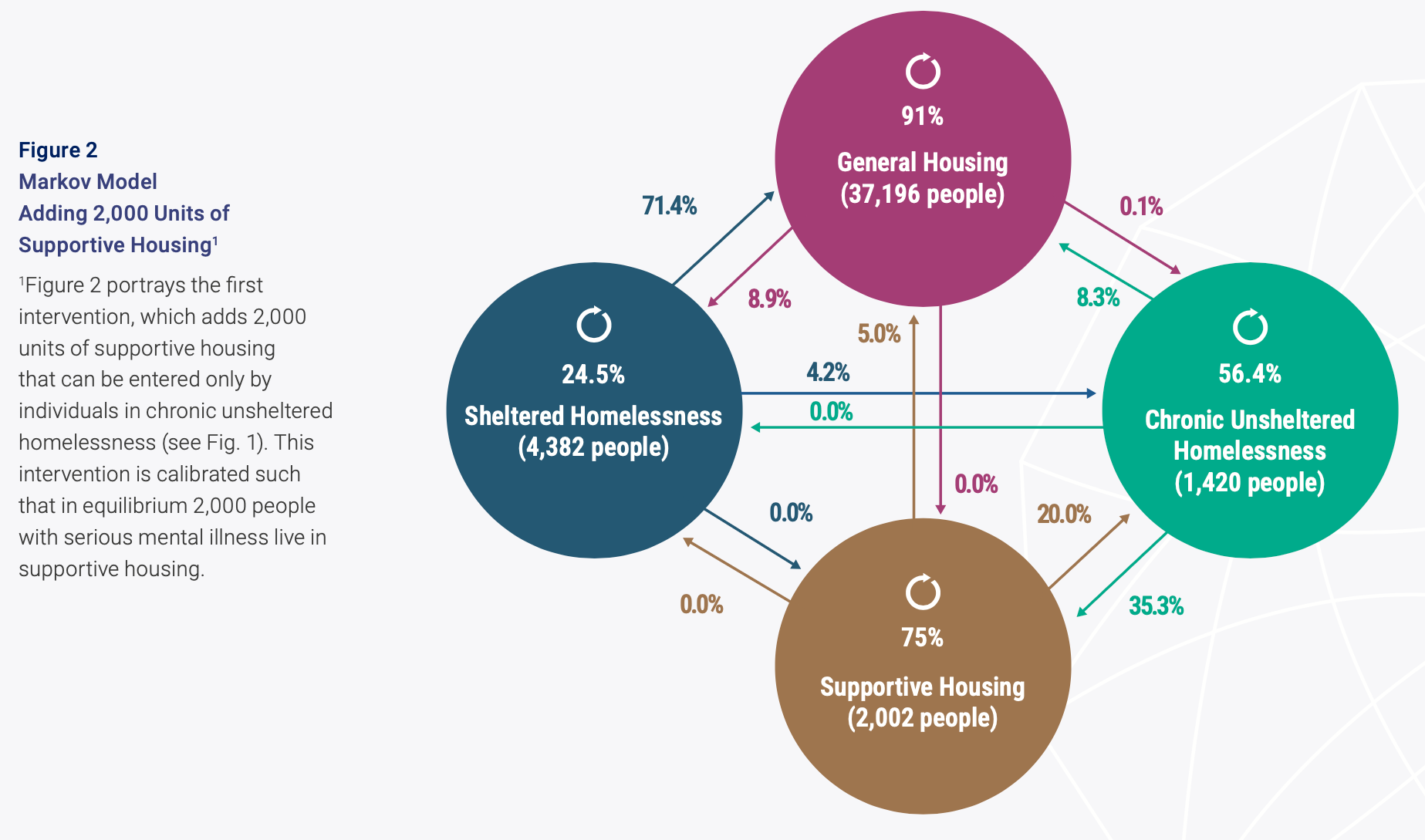
Next, we modeled the effects of adding 2,000 units of new supportive housing (Fig. 2) and of supplementing that housing with additional interventions (Fig. 3). We modeled the effect of adding housing by modifying our base case transition rates, shifting 2,000 people from chronic homelessness into supportive housing by applying a 35.5% transition rate from chronic unsheltered homelessness into housing. We assumed that among those in these new supportive housing units, 75% remain in supportive housing while 20% return to the street and 5% move to the general housing state. The figures in the bubbles (Fig. 2) show the steady-state outcomes under these assumptions. The intervention reduced the number in chronic unsheltered homelessness in the steady state by FIG 2 approximately 1,077, from 2,497 to 1,420; that is, the reduction in the chronic unsheltered census is a little more than half the number of new units added.
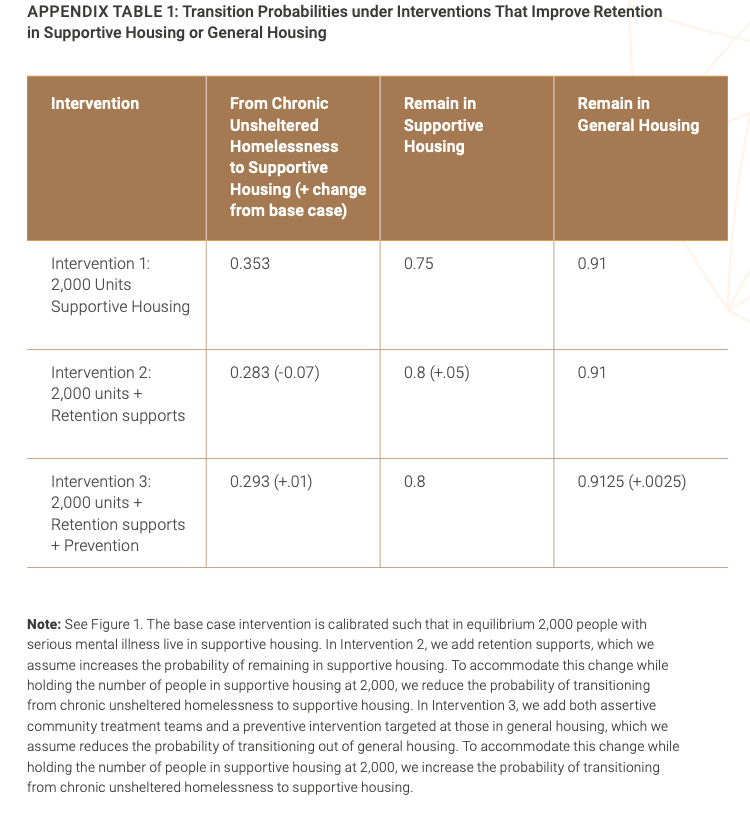
In Figure 3, we show the effect of this new supportive housing supplemented by two interventions: a retention program that increases the percentage of individuals remaining in supportive housing and a preventive program that reduces the percentage of housed individuals who lose their housing. Table 1 in the Supplement describes the modifications of transition probabilities we used to describe these interventions. We assumed that adding retention supports (intervention 2) increased the share of people who remain in supportive housing from one year to the next by 5%.
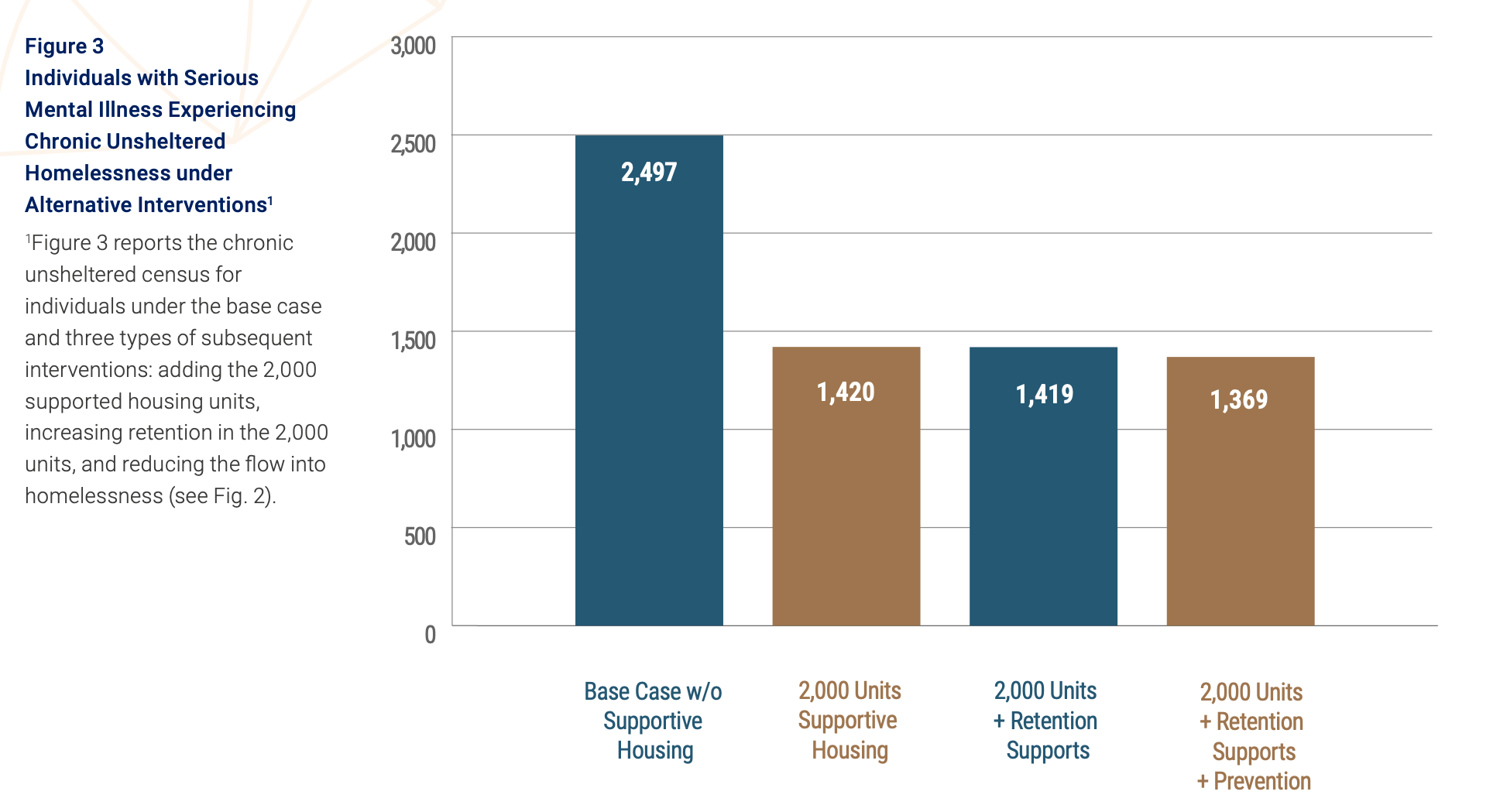
As Figure 3 shows, in the base case, adding 2,000 units of housing reduced the number of people with serious mental illness who are chronically unsheltered by 1,077 to 1,420, a 54-person reduction per 100 permanent supportive housing units added. Adding retention supports serving the same population has a negligible impact on the chronic unsheltered census if the number of supportive housing units is fixed. Adding preventive interventions that keep people from transitioning into chronically unsheltered homelessness, by contrast, is more effective in reducing chronically unsheltered homelessness, because a fixed number of units would be serving a smaller population.
Sensitivity Analyses
In Figure 4, we report the results of varying the stringency of targeting by allowing transitions from shelters into supportive housing. Even a small decline in targeting substantially reduces the number of people who are moved out of chronically unsheltered homelessness for a given supply of supportive housing. Under a slightly less stringent targeting strategy, more than three units of housing are needed to reduce the chronic unsheltered census by one person.
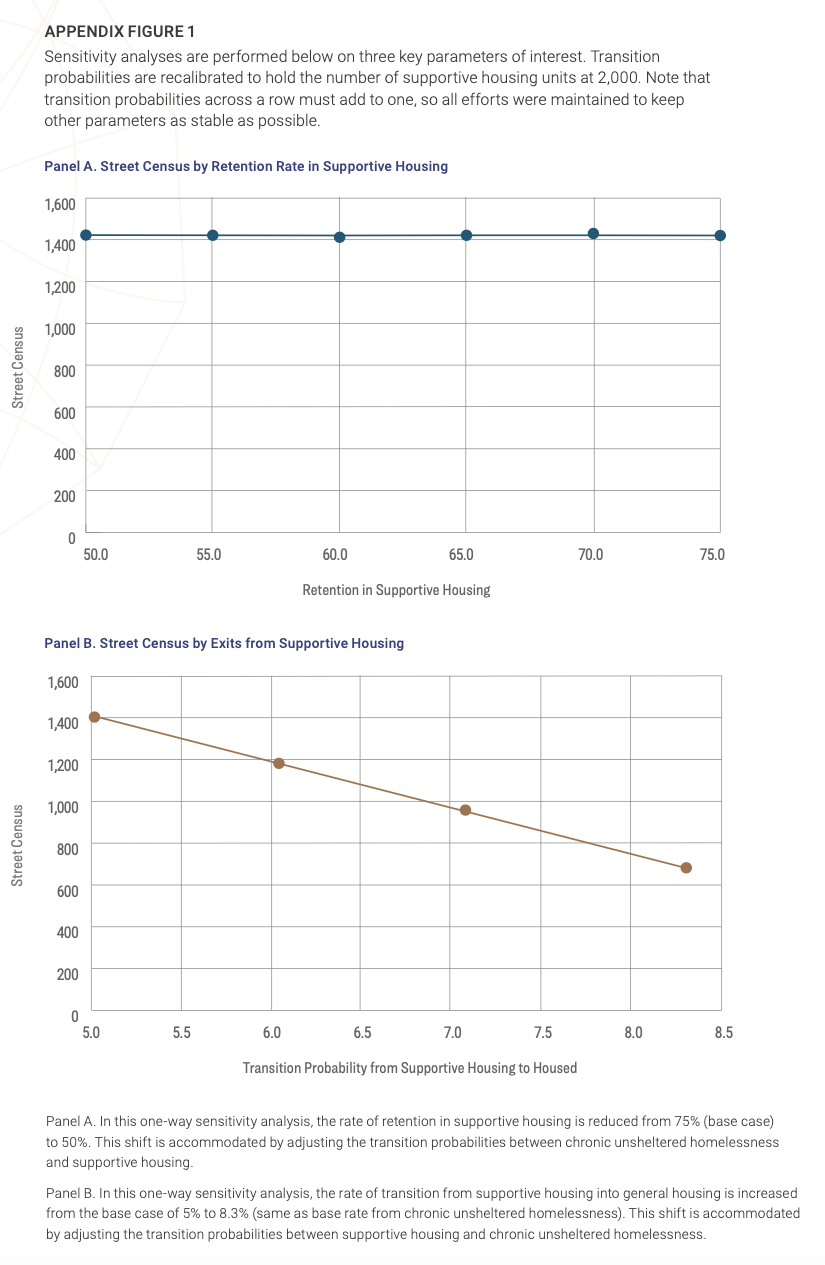
In Panel A in the Supplement we varied the rate of retention in supportive housing from the base case (25% leave supportive housing) to 50% leaving supportive housing each cycle/year. This assumption has little impact on the estimated number of people who are living in chronic unsheltered homelessness at a point in time: more people experience briefer episodes of living in the fixed number of supportive housing units. In Panel B, we varied the rate at which residents of supportive housing move into the general housing state (general housing, institutionalization, or mortality) from the baseline rate of 5% up to the rate for those who remain in chronic unsheltered homelessness (8.3%). Under this assumption, a given number of supportive housing units yields greater reductions in the number of people in chronic unsheltered homelessness. Because this may be due to higher mortality or institutionalization (which are included in the general housing state), however, this result could imply a loss in the well-being of the population.
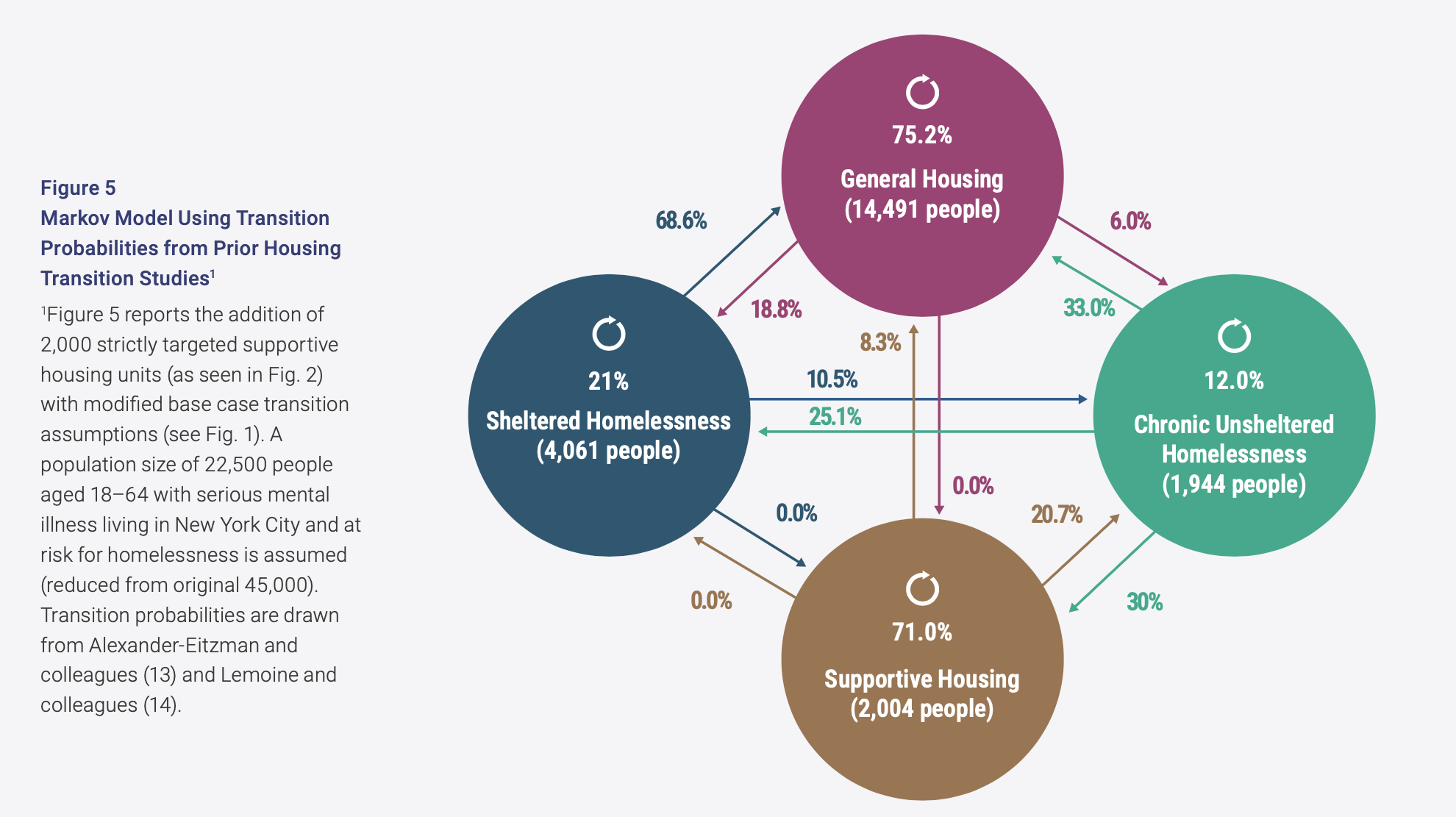
Finally, we modified all our baseline assumptions about transition (2,002 people) probabilities to more closely replicate the rates described in prior studies (Fig. 5). Under the rates of transition into and out of homelessness identified in prior supportive housing studies, four units of supportive housing are needed to reduce the chronic unsheltered census by one person.
Limitations
We grounded our transition rate assumptions on estimates of the PIT homeless population and on prior studies. However, the PIT estimates are highly uncertain, and the populations examined in prior studies had lower rates of serious mental illness than in the chronically unsheltered population we focused on. There are no published studies measuring many of the transition probabilities we used. We performed sensitivity analyses, checked for internal consistency, and calibrated to external data where available. The general patterns we observed are robust to substantial changes in the underlying assumptions.
5 Discussion
Our analysis highlights the importance of accounting for dynamics in addressing the difficult problem of people with serious mental illness who are chronically unsheltered. Our results reinforce the intuition that the most important intervention for getting homeless people into housing is housing. But accounting for dynamics implies that the amount of housing needed to reduce the chronically unsheltered homeless census is much greater than implied by the steady-state (or point prevalence) number of people who need to be housed.
Our model generated three key findings. First, even under very restrictive assumptions, about two new supportive housing units targeted to people who are chronically unsheltered are required to reduce this population by one person in steady state. Even this estimate is more favorable than some prior estimates. O’Flaherty (15) and Corinth (34) estimated a street reduction of just 10–20 individuals per 100 new beds across all unsheltered populations.
Our analysis highlights the importance of accounting for dynamics in addressing the difficult problem of people with serious mental illness who are chronically unsheltered.
The high number of units needed occurs because, inevitably, some share of additional units will house people who would otherwise have found other types of housing, or become institutionalized, or died. To the extent that supportive housing substitutes for institutionalization or mortality, the units are doing a great deal of good, even though the count of chronically unsheltered homeless people does not change very much (35). To the extent that supportive housing substitutes for general housing, the gain is somewhat smaller, though these units nonetheless support very disadvantaged people who might otherwise be living in challenging and substandard circumstances (36).
To the extent that supportive housing substitutes for institutionalization or mortality, the units are doing a great deal of good, even though the count of chronically unsheltered homeless people does not change very much.
Second, adding supplementary services for people in supportive housing or on the streets helps people remain in housing, but if the supply of housing is fixed, it does not have a very big effect on the number of people experiencing chronic unsheltered homelessness. Adding services that improve retention helps reduce the chronic unsheltered census only if more housing units are also made available.
Third, the number of supportive housing units needed to reduce the chronic unsheltered census is highly sensitive to the stringency of targeting. If people experiencing intermittent homelessness (and have higher rates of transition out of homelessness) are permitted to move into supportive housing units, far more units will be needed to reduce the census. In our sensitivity analyses, we found a result similar to that of O’Flaherty (15) and Corinth (34) if approximately 1.5% of those in shelters are permitted to enter supportive housing. This result does not require that people seeking housing behave strategically; it is simply an outgrowth of providing housing to people with higher underlying transition probabilities.
6 Conclusion
Adding supportive housing targeted to people with serious mental illness who are chronically unsheltered can help a very vulnerable population and reduce the chronic unsheltered census. But failing to account for the dynamics of homelessness can lead to results that disappoint proponents of housing programs. It is important to be realistic about how many units are likely to be needed and how strictly they will need to be targeted and resourced to achieve visible gains.